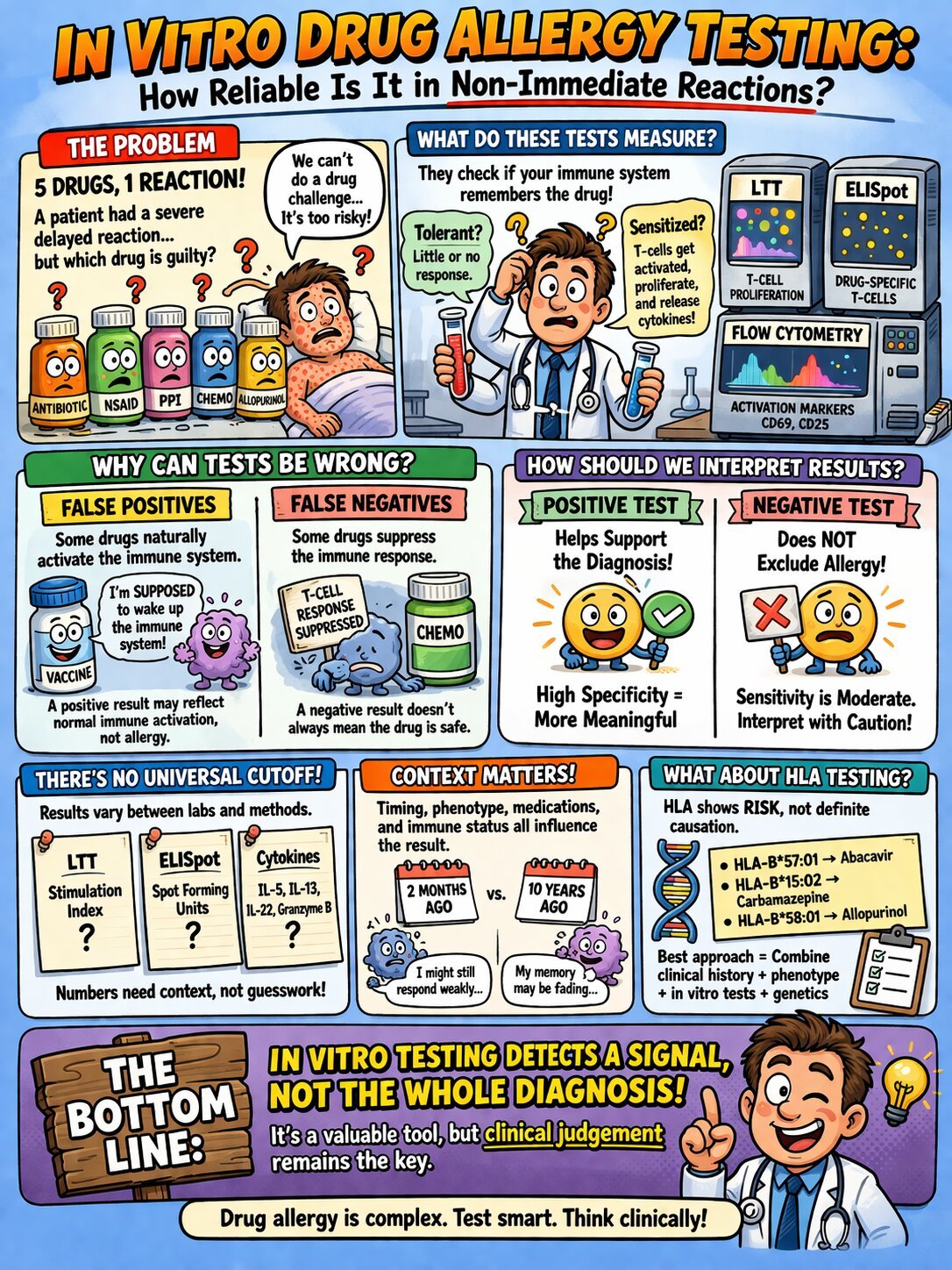
Drug allergy testing in non-immediate reactions is one of the most challenging areas in clinical practice, one of the most difficult situations is a patient with a severe delayed reaction and several possible culprit drugs. Drug allergy testing using in vitro methods is increasingly used when drug provocation is unsafe.
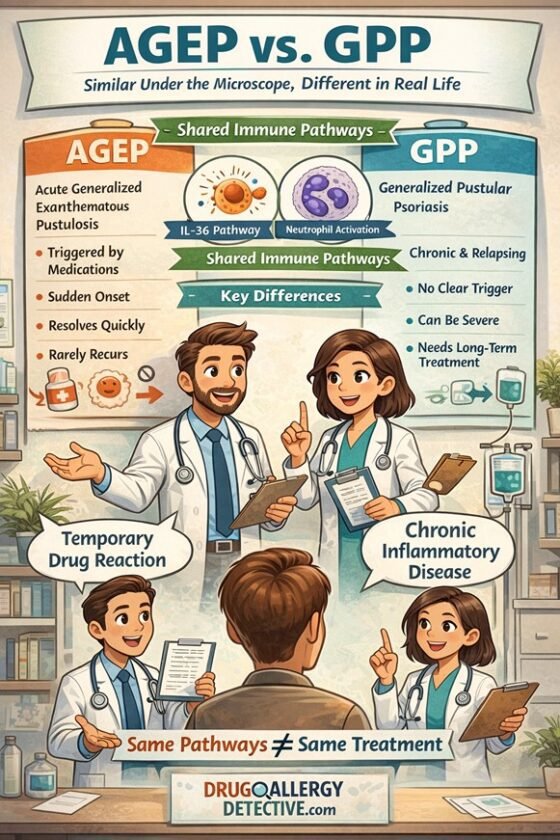
This is especially true in severe cutaneous adverse reactions (SCARs) such as Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN), drug reaction with eosinophilia and systemic symptoms (DRESS), and acute generalized exanthematous pustulosis (AGEP).
In these cases, drug provocation testing is often unsafe or unacceptable. The natural next step is to consider in vitro testing for drug allergy.
But an important question comes first:
How reliable are in vitro tests for non-immediate drug allergy, and what do they really tell us?
The short answer is this: these tests can be helpful, sometimes very helpful, but they do not provide a definitive diagnosis on their own. They detect immune reactivity, not necessarily clinical causality.
That distinction is central to proper interpretation.
What Is Drug Allergy Testing in Non-Immediate Reactions?
In vitro drug allergy testing refers to laboratory assays performed outside the body, usually using the patient’s peripheral blood mononuclear cells (PBMCs), to look for evidence of a drug-specific immune response.
In delayed drug hypersensitivity, the main target is usually the T-cell response.
The immunological principle is simple:
If a patient has been sensitized to a drug, drug-specific T cells may retain memory of that exposure. When those cells are re-exposed to the suspected drug in the laboratory, they may show:
- activation
- proliferation
- cytokine release
By contrast, cells from a tolerant individual may show little or no response.
This concept is elegant. In clinical practice, however, interpretation is far more complicated.
A laboratory signal of immune reactivity does not automatically prove that the drug caused the reaction in real life.
Why In Vitro Drug Allergy Testing Matters in Non-Immediate Reactions
In many cases of delayed drug allergy, clinicians need more than history alone.
This is particularly true when:
- the patient was exposed to several drugs at the same time
- the reaction was severe
- re-exposure would be high risk
- the future treatment plan depends on identifying the culprit accurately
That is why drug allergy blood tests such as lymphocyte transformation testing (LTT) and ELISpot assays attract so much interest.
They offer the possibility of narrowing the list of suspect drugs without putting the patient back at risk.
But they also come with important limitations.
Which In Vitro Tests Are Used in Non-Immediate Drug Allergy?
Several assays are used in the evaluation of non-immediate drug hypersensitivity. They are not interchangeable, and the level of clinical validation differs across methods.
1. Lymphocyte Transformation Test (LTT)
The lymphocyte transformation test measures T-cell proliferation after in vitro re-exposure to a suspected drug.
Methods may include:
- radiolabeled thymidine incorporation
- CFSE dilution
- BrdU-based assays
Results are usually expressed as a stimulation index.
The LTT is one of the best-known in vitro assays in this field, but its sensitivity is variable. Performance may depend heavily on the timing of testing, the drug involved, and the clinical phenotype.
2. ELISpot and Cytokine-Based Assays
ELISpot drug allergy testing detects cytokine release from drug-reactive T cells.
The most commonly studied marker is interferon-gamma (IFN-γ), but other cytokines and mediators have also been explored, including:
- IL-5
- IL-13
- IL-22
- granzyme B
These assays may be particularly useful in some severe delayed reactions, including SCARs. In many settings, they appear to offer relatively high specificity, but there is no universal cutoff and no single cytokine profile that works across all drugs, all reactions, and all laboratories.
3. Flow Cytometry-Based Activation Marker Assays
Flow cytometry can be used to detect T-cell activation markers such as:
- CD69
- CD25
These assays may capture early immune activation, but they remain less standardized for routine clinical use than LTT or ELISpot in most centers.
At present, they are better viewed as promising tools than as fully mature routine diagnostics.
How Reliable Is Drug Allergy Testing?
This is the key clinical question.
The answer is not a simple yes or no.
In general, in vitro testing for drug allergy tends to be more useful when positive than when negative.
That is because many assays in this field show a familiar pattern:
- specificity may be relatively high
- sensitivity is often only moderate or low
In practical terms:
- a positive result may support causality
- a negative result does not reliably exclude allergy
This asymmetry is one of the most important principles in interpreting drug allergy blood tests.
Why In Vitro Drug Allergy Tests Can Be Misleading
Limitations of Drug Allergy Testing in Delayed Reactions
Even well-performed assays can produce results that are biologically real but clinically misleading. In clinical practice, drug allergy testing results must always be interpreted cautiously.
False Positives
Some drugs are immunogenic by design or can activate the immune system in ways that do not represent classical drug allergy.
Examples include:
- vaccines
- immune checkpoint inhibitors
A positive in vitro result in these settings may reflect expected immune activation rather than true hypersensitivity.
In other words, the test may detect a real response, but not the kind of response that proves clinical allergy.
False Negatives
False negatives are at least as important, and often more dangerous.
Some drugs suppress the very response the assay depends on. This is particularly relevant for:
- chemotherapy agents
- immunosuppressive drugs
- systemic corticosteroids
This matters enormously in SCARs, because many patients with severe reactions receive corticosteroids during the acute phase. If testing is performed too early, or while immune suppression is still relevant, the result may look negative even though the patient truly is allergic.
A negative result in that situation may reflect suppressed assay responsiveness, not absence of drug-specific immunity.
Sensitivity Is Often Overinterpreted
There is another important limitation.
In severe reactions such as SJS/TEN, DRESS, and AGEP, a true gold standard is usually unavailable because drug rechallenge is often ethically impossible.
That means test performance is commonly evaluated against clinical history, not against definitive proof.
So what is often reported as “sensitivity” may be closer to a detection rate against a clinical surrogate than a true measure of diagnostic accuracy.
That does not make the literature useless. But it does mean results should be interpreted with caution.
What Does a Positive Drug Allergy Blood Test Mean?
A positive in vitro test suggests that the patient’s immune cells responded to the drug under laboratory conditions.
That can be clinically useful.
In the right context, a positive result may:
- strengthen suspicion for a culprit drug
- help narrow the differential diagnosis
- support avoidance of a specific agent
- guide decisions when several drugs are possible culprits
But even a positive result should not be interpreted in isolation.
Clinicians still need to ask:
- Does this fit the phenotype?
- Does the timing make sense?
- Could the drug itself be broadly immunogenic?
- Was the assay performed under valid conditions?
So a positive test may support causality, but it does not automatically prove it.
What Does a Negative Drug Allergy Test Mean?
This is where mistakes often happen.
A negative in vitro result simply means that no relevant immune reactivity was detected under the conditions of that assay.
It does not necessarily mean:
- the patient is not allergic
- the suspected drug is safe
- the diagnosis has been excluded
Negative results may occur because of:
- low assay sensitivity
- poor timing of testing
- recent corticosteroid exposure
- chemotherapy or immunosuppressive treatment
- phenotype-specific biology
- drug-specific limitations of the assay
For severe delayed reactions, especially SCARs, a negative result should be interpreted very cautiously.

Why There Is No Universal Cutoff in In Vitro Drug Allergy Testing
Many clinicians are familiar with standardized thresholds in other forms of allergy testing. In vitro drug allergy testing does not work that way.
Depending on the assay, interpretation may rely on:
- stimulation index in LTT
- spot-forming units in ELISpot
- cytokine concentrations in supernatants
- activation marker expression by flow cytometry
These values vary across:
- laboratories
- protocols
- timing windows
- drug classes
- reaction phenotypes
A numerical threshold reported in one study cannot simply be transplanted into another laboratory’s workflow.
That is why numbers alone should never drive the diagnosis.
Why Timing Matters in Non-Immediate Drug Allergy Testing
Timing is one of the most underappreciated factors in delayed drug hypersensitivity testing.
The same laboratory result may carry very different meaning depending on when the patient is tested.
For example:
- a weak ELISpot response 10 years after the reaction may still be meaningful
- the same weak response 2 months after a severe SCAR may be unexpectedly low and raise concern about suppression or suboptimal timing
Timing matters because immune responses evolve. So do the effects of treatment.
This is one reason clinical context matters more than the number alone.
What Factors Affect Interpretation of In Vitro Drug Allergy Tests?
No test result should be interpreted outside the broader clinical setting.
Important factors include:
1. Timing of Testing
Testing too early, especially after severe DRESS reactions, may reduce sensitivity.
2. Corticosteroid Exposure
Recent or ongoing steroid use may suppress proliferation and cytokine release.
3. Reaction Phenotype
DRESS, SJS/TEN, and AGEP do not behave identically and may show different assay performance profiles.
4. Immune Status
Immunocompromised patients and patients receiving immunomodulatory therapy require especially cautious interpretation.
5. Drug Class
Assay performance may differ substantially between anti-tuberculosis drugs, sulfonamides, anticonvulsants, chemotherapy agents, and other drug classes.
This is why interpreting in vitro drug allergy testing is not just about laboratory technique. It is also about understanding the biology of the patient, the drug, and the reaction.
Can Assay Sensitivity Be Improved?
This is an important area of ongoing research.
One strategy is assay augmentation, designed to overcome immune suppression that may cause false-negative results.
For example, anti-PD-L1 blockade has been explored as a way to restore suppressed T-cell responses in IFN-γ ELISpot testing, particularly in patients who received corticosteroids.
This is not yet standard routine practice, but it illustrates an important point:
The field is evolving, and researchers are actively trying to improve the sensitivity of in vitro testing for drug allergy in real-world patients.
What Is the Role of HLA Testing in Non-Immediate Drug Allergy?
Some severe delayed drug reactions are strongly associated with specific HLA alleles.
Important examples include:
- HLA-B*57:01 and abacavir hypersensitivity
- HLA-B*15:02 and carbamazepine-associated SJS/TEN in certain Asian populations
- HLA-B*58:01 and allopurinol-associated SCAR
These are among the most important pharmacogenomic associations in clinical medicine.
But HLA testing also has to be interpreted correctly.
HLA testing identifies risk, not definitive causality.
A patient may carry a risk allele and never react. Another patient may have a convincing reaction despite absence of the best-known allele.
So HLA testing is valuable, but it should be integrated with:
- clinical history
- reaction phenotype
- in vitro test results
- overall diagnostic reasoning
Can In Vitro Testing Diagnose Non-Immediate Drug Allergy by Itself?
No.
That is the most important bottom-line answer.
In vitro drug allergy testing does not diagnose non-immediate drug allergy on its own.
It detects a signal of immune reactivity.
That signal may be:
- clinically relevant
- clinically misleading
- suppressed
- amplified
- difficult to interpret without context
The final diagnosis still depends on clinical judgment.
Clinical Takeaway
For clinicians evaluating non-immediate drug allergy:
- a positive in vitro test may meaningfully support causality
- a negative test should not be used alone to exclude allergy
- timing, phenotype, immune status, and recent treatment all matter
- HLA testing adds important risk information, but does not replace clinical interpretation
The best approach is an integrated one.
The Bottom Line
In vitro testing for drug allergy is useful, but it is not definitive.
In non-immediate reactions, especially SCARs, these assays can help identify culprit drugs when provocation testing is too dangerous. But they do not provide a simple yes-or-no answer.
They measure immune reactivity, not necessarily clinical causality.
That is why the real diagnosis still comes from the combination of:
- clinical history
- reaction phenotype
- timing
- laboratory findings
- genetics when relevant
- careful clinical judgment
Non-immediate drug allergy is complex, time-dependent, and context-sensitive. No single laboratory test can fully capture that complexity. Drug allergy testing remains a valuable tool, but not a definitive diagnostic method.
Suggested Readings
This article is intended as a clinical educational resource. Specific assay protocols, cutoffs, and clinical recommendations should be evaluated in the context of local laboratory capabilities and the evolving primary literature.